Nursing records provide information about the care provided and ensure communication between professionals involved in care, with the aim of clearly reporting the needs of patients and the progressive assessment of the patient's condition.
However, there are still flaws in the implementation of Nursing Records, such as the use of wrong termologies, the absence of important items about the patient's condition and the use of non-standardized acronyms, which contributes to insufficient data for the complete assessment of the patient.
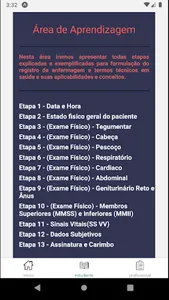
The application is able to recall the steps of the physical examination, exemplify and describe them, in addition to having the function of creating a record model based on the information collected by the nursing professional
However, there are still flaws in the implementation of Nursing Records, such as the use of wrong termologies, the absence of important items about the patient's condition and the use of non-standardized acronyms, which contributes to insufficient data for the complete assessment of the patient.
The application is able to recall the steps of the physical examination, exemplify and describe them, in addition to having the function of creating a record model based on the information collected by the nursing professional
Show More